Middle Ear Infections in Children
Details of the condition
GLUE EAR AND MIDDLE EAR INFECTIONS
- Glue ear and recurrent acute otitis media are part of the same spectrum of suppurative otitis media, and as such are considered together.
- It is possible for the presenting complaint to be with glue ear (hearing loss) or recurrent ear infections (pain/ fever) by themselves, or these problems can occur together.
- When the symptoms are severe and persistent over a prolonged period for any of these clinical scenarios, grommet insertion becomes an option.
WHAT IS MIDDLE EAR INFECTION?
- Acute otitis media is a painful infection of the ear which is common in young children.
- It usually follows a viral infection, and probably relates to secondary infection from bacteria including Streptococus pnumoniae, and Haemophilus influenzae.
- A few middle ear infections per year may be part of normal development, and are usually treated with antibiotics.
- If infections are too frequent, then grommet insertion is likely to help the situation.
WHERE IS YOUR MIDDLE EAR?
- The middle ear is normally an air-filled space between the ear drum and the inner ear (cochlea).
- It contains the bones of hearing which connect the ear drum to the inner ear.
- Infections enter the middle ear form the back of the nose via the eustachian tube, causing pain, fever and loss of hearing. The ear fills with pus.
- If the eustachian tube is blocked over a prolonged period, the middle ear fills with thick mucus (“glue ear”) causisng hearing loss, because the ear drum cannot vibrate properly
WHAT IS THE DIFFERENCE BETWEEN A MIDDLE EAR INFECTION AND GLUE EAR?
- A middle ear infection – is associated with significant pain, fever and an unwell child. It represents an abscess (pus) behind the eardrum.
- Glue ear – can occur after an infection, or can occur without a clear history of ear infection. It thick mucus, or golden fluid behind the ear drum It is not painful, and the child is well. It is associated with hearing loss.
WHEN DO MIDDLE EAR INFECTIONS OCCUR?
- Middle ear problems are experienced at some stage by majority of children.
- There is a natural fluctuation of middle ear issues, related to the seasons, and an improvement with age (seen between 4-6 for most children).
HOW DO EAR INFECTIONS AFFECT YOUR HEALTH?
- Too many infections leave a child constantly having fevers, being run down, sleeping poorly and requiring multiple trips to the doctors and courses of antibiotics.
- Ear infections are very disruptive to lives of children and their families who often have to take a lot of time out of their routine schedule, with time off kindy, school or work
SYMPTOMS OF MIDDLE EAR INFECTIONS?
- Pain
- Fever
- Reduced hearing
WHAT ARE THE BEHAVIOURAL INDICATIONS OF EAR INFECTION?
Ear symptoms can vary with age but behaviour associated with a painful middle ear in a young child can include:
- Abnormal irritability
- Feeding difficulties
- Consistent presence of fever
- Ear tugging
- Disturbed sleep.
- A miserable and unwell child
HEARING LOSS SYMPTOMS ASSOCIATED WITH MIDDLE EAR INFECTION
- Typically, glue ear will present as a mild-to-moderate hearing loss, similar to walking around with your fingers blocking your ears.
- The best possible hearing in children is often substantially better than what is considered “normal“ in the adult population. This mean there is a degree of reserve.
- A child’s hearing will typically still hear one-on-one but will struggle in more challenging auditory environments.
- In many cases, the hearing loss is very obvious to parents, carers and teachers.
WHAT ARE THE STAGES OF A MIDDLE EAR INFECTION?
- The first stage is pain and fever
- The acute infection may:
- Resolve spontaneously with time, with the ear returning to normal.
- Resolve with the help of antibiotics
- Burst the ear drum with pus discharge from the ear. In most cases the pain will then improve, and the hole in the ear drum will heal.
- The infection may settle, but the patient is left with glue ear (thick mucus behind the ear drum), which causes hearing loss
WHAT ARE THE CONSEQUENCES IF UNTREATED EAR INFECTION?
- In rare cases where no action is taken there may be severe compolications including meningitis and brain abscess.
- There may be permanent structural damage to the ear drum if multiple recurrent ear infections occur without appropriate treament.
- If infections are too frequent or too severe, antibiotics are no longer enough and grommets will be required to improve the child’s wellbeing.
WHAT ARE THE CAUSES OF MIDDLE EAR INFECTIONS
- Children have immature eustachian tubes and immune systems leaving them more susceptible to the upper respiratory infections which we all encounter throught the year.
- This sets the scene for a secondary infection with nasty bacteria (eg Streptococci, Haemophilus) which cause ear infections.
- Children become less prone to infections once they reach school age (4-6).
- For the worst cases ear infections may continue beyond this age group.
MY CHILD GETS A LOT OF EAR INFECTIONS. HOW MANY EAR INFECTIONS ARE TOO MANY?
- Most young children will have ear infections from time to time. This is more common when they are in kindergarten or day care, and over the winter months.
- Once the infections are “back to back”, with frequent antibiotics and visits to the local doctor consideration should be given to a specialist ENT referral.
- There may be associated hearing loss with glue ear, and part of the assessment will probably include a hearing test.
- In the circumstance of severe recurrent ear infections, grommet insertion can dramatically improve your child’s quality of life and substantially reduce the requirement for antibiotics.
HOW DO THE MIDDLE EAR INFECTIONS AFFECT YOUR CHILD’S HEALTH?
Impact from Middle Ear Infection can include:
- Delay in educational development.
- Frequent middle ear infections cause ongoing misery for a child and their family.
- Lifelong problems caused by hearing loss
DIAGNOSIS OF MIDDLE EAR DISEASE
Middle ear disease can be diagnosed by your doctor when the history is taken. Middle ear disease is indicated when a child presents with:
- ear pain
- fever
- unsettled child, poor sleep
- deafness
- language delay
- other ENT symptoms such as blocked nose, thick snot, cough , tonsillitis, snoring
During an examination your doctor will possibly see:
- characteristic red, swollen ear drum in middle ear infections (below)

Figure: the red drum of acute otitis media
- golden or dull ear drum with fluid

WHY HAS A HEARING TEST BEEN RECOMMENDED?
- Hearing testing is routine in children with suspected middle ear problems, and helps to predict which children would be helped by an operation.
- Various hearing tests can determine if there is hearing loss at a level that will compromise a child’s educational development.
TESTING THE EAR WITH MIDDLE EAR INFECTION OR MIDDLE EAR FLUID TYMPANOMETRY
- Tympanometry tests the condition and function of the middle ear. It is not a hearing test.
- It measures the energy transmitted through the eardrum (tympanic membrane) to the conduction bones by creating variations of air pressure in the ear canal.
- The test assesses the presence of abnormal pressure behind the eardrum.
- Tympanometry is helpful in making the diagnosis of middle ear fluid build up (effusion).
- It is a useful screen for children who may have hearing loss.
AUDIOMETRY
Visually reinforced audiology
- Audiometry is a test to determine hearing levels or hearing loss. The test It will normally take 15 minutes to half an hour.
- We use distraction devices like the dancing puppet which makes the hearing test an enjoyable game for young children.
- Paediatric Visual Reinforcement Audiometry (VRA), or the Puppet Show Test is used with infants from 6 months up to children of 2 years.
- The puppet makes the hearing test like a game. The puppet will do an amusing dance if the child responds to a sound stimulus correctly.
- VRA is in a sound field meaning it tests the overall function of both ears together, rather than each ear separately.
Ear specific audiology
- In children older than 2 years, it is usually possible to test the ears individually.
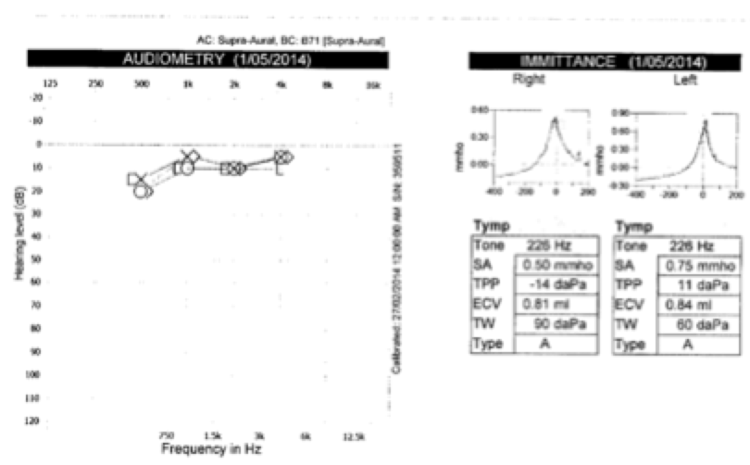
Figure: a hearing test of both ears confirming normal midle ear function and hearing in both ears for a 3 year old
Otoacoustic emissions
- This provides a pass/ fail test of overall ear function, and can be useful in very young children.
- A pass gives reassurance about normal middle and inner ear function.
- A fail is most commonly related to middle ear fluid
TREATMENTS FOR MIDDLE EAR INFECTIONS
- When patients present with persistent fluid or recurrent Middle Ear Infections there are a number of common courses of action. These are typically either:
- Watchful Waiting
- valsalva- eg EarPopper device
- Allergy treatment (spray such as nasonex)
- Long term, low dose antibiotics
- Grommet insertion
- When there is a history of multiple ear infections or persistent middle ear fluid with hearing loss, it is likely that an Ear, Nose and Throat (ENT) specialist will be involved in care.
WATCHFUL WAITING FOR RECURRING MIDDLE EAR INFECTION
- Usually middle ear infections are self-limiting and may require nothing more than clinical monitoring or the occasional course of antibiotics.
- The “wait and see” approach in some cases is advised. This approach acknowledges both the seasonal fluctuation in symptoms, and that most children have less symptoms as they get older.
- Improvement in middle ear infections normally, but not always, commences in the 4-6 year old age group.
ALTERNATE APPROACHES FOR MIDDLE EAR INFECTIONS
- There is no good evidence for any treatment other than grommets for persistent Middle Ear Infections, but other treatments are:
- Nasal Allergy Treatment may have some benefit, when allergic rhinitis is an issue in its own right. Using nasal sprays such as Nasonex may have a role.
- Inflation of the middle ear
- Using an EarPopper has some evidence for efficacy but can be difficult for children to tolerate.
- It is a device that pumps pressure into the Eustachian tube via the nose has some evidence, especially in adults but is not tolerated by many young children.
- Antibiotic Therapy – Long-term antibiotics have limited evidence, and carry potential issues with sideffects and antibiotic resistance.